Diagnosis (confirm with the same test on another day)
Symptoms of diabetes
· Polyuria
· Polydipsia
· Weight loss
· Nocturia
· Polyphagia
· Blurry vision
· PLUS random plasma Glucose ε 11.1 mmol/L (200 mg/dL) OR FBS ε 7.0 mmol/L (126 mg/dL) OR plasma glucose value ε 11.1 mmol/L (200 mg/dL) during two hour OGTT

Diagnostic testing
• Fasting blood glucose (FBG): best drawn the morning after overnight fast
• Oral glucose tolerance test (OGTT): 75 g glucose ingested, then plasma glucose levels measured following 0 and 120 minutes
 |
| Classification of Diabetes mellitus |
Diabetes Secondary to Specific Etiologies
1. Genetic
• Down syndrome, Turner’s syndrome, Huntington’s disease, genetic defects in ß-cell function and insulin action
2. Diseases of the endocrine/exocrine pancreas
• Pancreatitis, neoplasia, cystic fibrosis (CF), hemochromatosis (bronzed diabetes)
3. Endocrinopathies
• acromegaly, Cushing’s syndrome, glucagonoma, hyperthyroidism
4. Drug-induced
• ß-agonists, glucocorticoids, thiazides, phenytoin
5. Infections
• Cytomegalovirus (CMV), congenital rubella
Gestational Diabetes (GDM)
Glucose intolerance that develops during pregnancy
Incidence
• 2-4% of all pregnancies
Risk factors
• Age > 25 • member of high-risk ethnic group
• Obesity
• Previous GDM
• 1º relative with DM
• Previous macrosomic baby (> 4 kg)
Screening and diagnosis
• Any pregnant woman should be screened between 24 and 28 weeks
• 50 g glucose challenge test, measuring glucose one hour later
• If abnormal (7.8 mmol/L; 140 mg/dL), then 75 g oral glucose tolerance test (OGTT) should be done
• If any two of the following three values are met or exceeded, a diagnosis of GDM is established
• Fasting glucose ε 5.3 mmol/L (95 mg/dL)
• 1 hr value ε 10.6 mmol/L (190 mg/dL)
• 2 hr ε 8.9 mmol/L (160 mg/dL)
Fetus
Maternal hyperglycemia induces hyperinsulinemia in fetus results in macrosomia (insulin acts as a growth factor)
GDM: prone to respiratory distress, neonatal hypoglycemia, hypocalcemia, hyperbilirubinemia, polycythemia, and prematurity
Preexisting DM: all of the above plus intrauterine growth restriction (IUGR), sacral agenesis, cardiac structural defects
Mother
Increased risk of developing subsequent type 2 DM
Progression of diabetic retinopathy and nephropathy
Management
• Preconception care to normalize HbA1c (if preexisting DM)
• Tight glucose control (shown to decrease both fetal and maternal complications)
• Oral hypoglycemics contraindicated
• Insulin to maintain tight glycemic control if diet inadequate
• Fetus must be monitored carefully
Impaired Glucose Tolerance (IGT)
Diagnosis based on
• Fasting glucose 6.1-6.9 mmol/L (110-125 mg/dL)
• 2-hour OGTT 7.8-11.1 mmol/L (140-199 mg/dL)
1-5% per year develops DM
50-80% reverts to normal glucose tolerance
Weight loss may improve glucose tolerance
Associated with progressively greater risk of developing macrovascular complications
Complications of diabetes
The majority of complications involve the vascular system
Aggravating factors: poor glycemic control, inadequate control of hypertension and cholesterol, smoking, high fat diet
Macroangiopathy
accelerated atherosclerosis leading to coronary artery disease (CAD), stroke, pulmonary vascular disease (PVD) most common cause of death in type 2 DM
Microangiopathy
_ Major chronic complication of type 1 and type 2 DM
_ Path gnomonic lesion is basement membrane thickening
_ Classically causes retinopathy, nephropathy and neuropathy
_ Can involve many other organs, including heart and skin
1. Retinopathy
Epidemiology
• Present in 50% of patients after 10 years with DM
• One of the leading causes of blindness in North America
Types
• Non-proliferative (background)
• Generally no symptoms but may affect macula and impair vision
• Microaneurysms, hard exudates, dot and blot hemorrhages
• Pre-proliferative
• 10-40% progress to proliferative within one year
• Macular edema, venous shunts and beading, nerve fiber layer micro infarcts (cotton wool spots)
Proliferative
• Great risk for loss of vision
• neovascularization, fibrous scarring, vitreal detachment, retinal detachment
Presentation
• Asymptomatic to complete loss of vision
Prevention and management
• Tight glycemic control
• Photocoagulation (eliminates neovascularization)
• vitrectomy
• Frequent follow-up visits with an ophthalmologist (immediate referral after diagnosis of type 2 DM; in type 1, only after 5 years of DM
2. Nephropathy
Epidemiology
• Diabetes-induced renal failure is the most common cause of renal failure in North America
• 20-40% of persons with type 1 DM (after 5-10 years) and 4-20% with type 2 DM have progressive nephropathy
Presentation
• Initial changes include microalbuminuria, increased glomerular filtration rate (GFR) (up to 140%), enlarged kidneys
• Over 15 years, progresses to cause hypertension, persistent proteinuria (macroalbuminuria), nephrotic syndrome, renal failure
Prevention and management
• Tight glucose control
• Tight blood pressure control – ACE inhibitors (Shown to reduce nephropathic complications) and calcium channel blockers (CCB)
• limit use of nephrotoxic drugs and dyes
• Protein restriction (controversial)
3. Neuropathy
Epidemiology
• Common in both type 1 and type 2 DM
Pathophysiology
• Metabolic defect thought to be due to increased sorbitol and/or decreased myoinositol (exact mechanisms not understood)
Types
• Distal symmetric “glove and stocking” polyneuropathy
• Autonomic dysfunction (e.g. gastroparesis)
• Mononeuropathy (e.g. carpal tunnel syndrome)
Presentation
• Paresthesias or neuropathic pain
• Motor or sensory deficits (including cranial nerves)
• Orthostatic hypotension
• Impotence
• voiding difficulties
• Foot ulcers
Prevention and management
• Tight glucose control
• Anti-depressants (e.g. amitriptyline), capsaicin, and anti-epileptics (e.g. Tegretol, Neurontin) for painful neuropathic syndromes
• Erythromycin and domperidone for gastroparesis
• foot care education
4. Other Complications
· Skin disease
· Bone and joint disease
· Cataracts
Treatment of diabetes
Diabetes Control and Complications Trial (DCCT) (1993) demonstrated a 50-70% decrease in microvascular complications in type 1 DM in an intensively treated group as compared to a conventionally treated group
United Kingdom Prospective Diabetes Study (1998) demonstrated a
• Decrease in diabetes complications in intensively treated group compared to conventionally treated group
• marked decrease in vascular complications in those with
Well-controlled blood pressure
Diet
· Energy intake to achieve and maintain desirable weight
· Other recommendations as per Canada's Food Guide
Lifestyle
Regular physical exercise can improve insulin sensitivity and lower lipid concentrations and blood pressure
stop smoking and decrease alcohol consumption
Oral Hypoglycemic Agents
Mainly for type 2 DM

Clinical Pearl
· Sulfonyureas and Meglitimides “squeeze” endogenous insulin from the pancreas.
· Biguanides and Thiazolidinediones act primarily in peripheral tissues remote from the pancreas.
Insulin (see Table)
Doses adjusted for individual patient needs to meet target glycemic control
Administration
• Subcutaneous injections
• Continuous subcutaneous insulin infusion pump
• IV infusion (regular insulin only)
Preparations
• Ultra-rapid (Humalog)
• Rapid or regular (R or Toronto)
• Intermediate (N or NPH, L or Lente)
• Long-acting (U or Ultralente)
_ Multiple daily injections of different types of insulin usually necessary for optimal glucose control
_ Estimate of total daily insulin requirement when starting an adult type 1 diabetes patient on insulin = 0.5 - 0.6 units/kg


Glucose Monitoring
_ Frequent self-monitoring and recording of blood glucose is now standard management
_ Hemoglobin A1c (HbA1c or glycosylated hemoglobin)
• Percentage indicates level of plasma glucose over past 3 months
• Extremely useful for monitoring patient’s long-term diabetes control
• Goal is to maintain HbA1c within 5-8% range (i.e. average blood glucose 5.0-11.0 mmol/L)
• HbA1c ε 10% indicates poor control
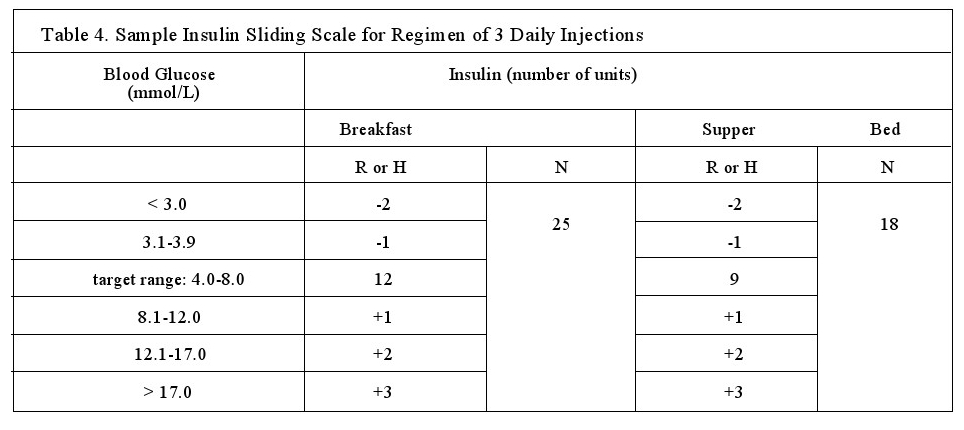
Variable Insulin Dose Schedule (“Sliding Scale”)
_ Patient takes fixed doses of intermediate-acting insulin (N) but varies doses of fast-acting insulin (R or H) based on blood glucose reading at time of dose
_ Use baseline R or H dose when in blood glucose target range; add or subtract units when above or below target
_ allows patient to make corrections to avoid long periods of hyper- or hypoglycemia
Insulin Pump Therapy
_ External, battery-operated pump continuously delivers basal dose of fast-acting insulin through small subcutaneous catheter
_ At meals, patient programs pump to deliver extra insulin bolus
_ Basal dose may be increased or decreased based on activity, sleep, etc.
_ Advantages: more flexible lifestyle (sleep in, eat / skip meals when desired), better glucose control
_ Disadvantages: very expensive, increased risk of DKA if pump inadvertently disconnected, frequent blood glucose testing required



No comments:
Post a Comment