Anatomical aspects
Liver is the largest visceral organ
Essential for life
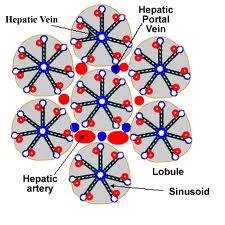
Hepatic lobule –Contains Central efferent hepatic venule with cords of hepatocytes and
sinusoids converging on to the venule.
Hepatic lobule –Contains Central efferent hepatic venule with cords of hepatocytes and
sinusoids converging on to the venule.
 |
| Arrangement of Liver cells |
Liver Acinus
Functional unit of liver.
Lie as parenchymal mass between 2 centrilobular veins.
Core of acinus contains portal triad
 |
| Liver acinus |
Acinus mainly consist of – 3 functional zones
Zone 1- Periportal
- Highest O2 consumption
- Highest metabolic rate
- Protein synthesis
- Secrete glucose into sinusoids.
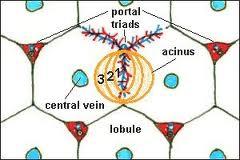
Zone 2 – mediolobular
Intermediate oxygen supply
Intermediate enzyme activity
Zone 3 - centrilobular
- Least oxygen supply
- High concentration cytochrome P-450
- Drug biotransformation
- Utilize glucose
Liver Sinusoids
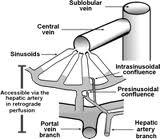
- Liver sinusoids are low pressure microcirculatory system
- Sphincters at hepatic arteriole, hepatic venous sinusoid and arteriolar portal shunts.
- Reservoir for blood
Types of Cells
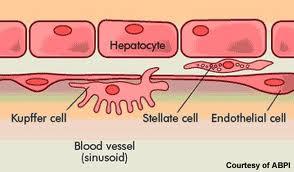 |
Cells of Liver
|
Functions of Liver
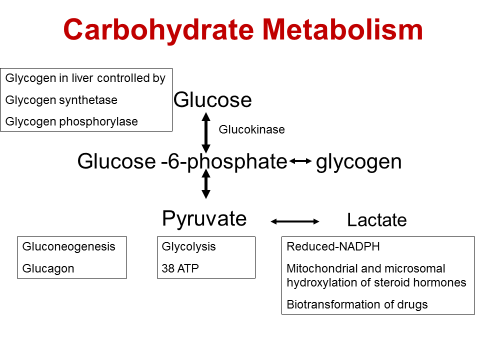
Carbohydrate metabolism
- Maintain blood glucose – glucose buffer function
- Stores glycogen
Glucose uptake
- Into portal venous system from gut– energy dependent active process
- Into hepatocyte from portal venous system - passive
Major components of Carbohydrate Metabolism handled by liver
- Glycogen synthesis
- Gluconeogenesis
- Glycolysis
- Reduced NADPH formation
Lipid Metabolism
Synthesis of fatty acids which are converted to triacylglycerol & VLDL
Partial oxidation of FA to ketone bodies
Cholesterol metabolism
80% converted to bile
20% bound to lipoprotein in blood
Bile production
At a rate of 1L/day.
Concentrated in gall bladder
Produce bile acids from cholesterol– cholic acid & chenodeoxycholic acid
Bile acids + glycine/taurine = bile salts
Bile salts - Emulsify dietary fat
Absorb fat soluble vitamins- A,D,E,K
Reabsorbed at terminal ileum- portal circulation- liver “enterohepatic circulation”
Bilirubin Metabolism
Formed in RES from haemoglobin
Transported to liver bound to albumin
Conjugated with glucuronide; secreted in bile
Conjugated bilirubin - Urobilinogen in gut
Protein Metabolism
Anabolism
Catabolism
Remove AA’s from blood for gluconeogenesis and protein synthesis
Release AA’s into blood for other tissues
Breakdown AA’s – remove N2 as urea
Protein Anabolism
AA’s & short peptides delivered to liver from gut
Synthesize
Albumin – 120-300mg/kgBW/day
α1, α2, β globulins – transport proteins
Haptoglobulin, α1 anti-trypsin, α2 macroglobulin, antithrombin III, α1 acid glycoprotein &
C reactive protein
Vitamin K dependent clotting factors – II, VII, IX, X
Vit K independent clotting factors – V, VIII, IX, XII, XIII
Purine & Pyrimidine bases
Protein Catabolism
Rate of protein turnover – 10 days
Muscle – 180 days
AA degradation by transamination, deamination and decarboxylation.
Produce acetyl CoA, oxyglutarate, succinyl CoA, fumarate – enter citric acid cycle
Urea synthesis
AA degradation ammonia – toxic
Converted to urea- in ornithine cycle
100 g protein – 30g urea
Creatine synthesis
Synthesized from methionine, glycine and arginine.
Phosphocreatine stored in muscle – back up energy
Phosphocreatine creatinine
Phagocytic function
By Kupffer cells
Infective, inflammatory and tissue injury substances
Phagocytosed material degraded by lysosomal enzymes
Storage functions
Glycogen
Triglycerides
Vitamins – A, D, E, K and B’s
Iron – excess as ferritin
Copper
Drug Metabolism
Eliminate exogenous and endogenous compounds
Lipophilic /partially ionised hydrophilic
2 phases
Phase I – oxidation, reduction, hydrolysis
Phase II- Glucuronidation, Sulphation, acetylation
Phase I
Increase hydrophilicity
Oxidative catalysed by cytochrome P-450 in smooth ER
Reductase & hydrolase – cytoplasm
Some products - active
Phase II
Occur In cytoplasm
Glucuronidation – glucuronosyl transferases
Most inactive products
Drug clearance affected by
Hepatic blood flow
Plasma protein binding
Enzymatic activity
Liver Blood Flow
1.5 L/min
25% of cardiac output
Hepatic artery & portal vein
Hepatic artery
30% total hepatic flow
40-50% total hepatic oxygen supply
Oxygen saturation 98%.
Pressure similar to systemic BP
High resistance in hepatic arteriole – pressure 35mmHg
Hepatic sinusoidal pressure 2 mmHg – due to ratio of pre sinusoidal/post sinusoidal resistance
Innervated muscular coat.
Portal vein
70% of liver blood flow
50-60% of basal oxygen supply
Oxygen sats – fasting state – 85%
increased gut activity – reduced
Valveless vein
Low pressure (5-10mmHg), low resistance, low velocity system
Hepatic veins
To IVC via R & L hepatic veins
Hepatic veno-constriction
- Norepinephrine
- Angiotensin
- Hepatic nerve stimulation
- Histamine
Hepatic venous pressure influenced by
- IPPV
- IAP
- Gravity
- Gut wall activity
Hepatic Microvasculature
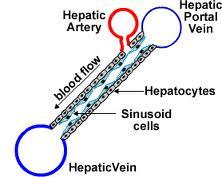
Sinusoid – formed by hepatic arteriole and portal venule
Flow to central vein
Pressure 2mm Hg.
Oxygen consumption increased by increased oxygen extraction at sinusoids.
Capacitance function
Reservoir volume 450ml
Mobilized in hypovolaemia by catecholamines.
Act as buffer against increased blood volume
Regulation
High blood flow
Increased oxygen demand leads to increased oxygen extraction ; not an increase in blood flow
- Intrinsic control
- Extrinsic control
Intrinsic control
Autoregulation
In hepatic artery
When pressure reduce flow is maintained by lowering resistance until SBP<80mmHg.
Portal vein
No autoregulation
Flow related linearly to pressure
Semi-reciprocal interrelationship
Reduction in portal venous blood flow increase hepatic arterial blood flow
by decreasing hepatic arterial resistance.
No change in portal venous blood flow with reduction in
hepatic arterial blood flow – no autoregulation
“Hepatic arterial buffer response”
Due to intrahepatic adenosine - Reduced portal blood flow –
adenosine build up- hepatic artery vasodilatation
Myogenic mechanism
Increased hepatic venous pressure increase hepatic arterial resistance and
decrease hepatic arterial blood flow.
eg. CCF
Extrinsic Control
Hepatic artery – α & β adrenergic receptors & dopamine receptors
Portal vein – α adrenergic & dopamine receptors
Epinephrine –
- Portal venous constriction
- Initial vasoconstriction followed by vasodilatation of hepatic artery
Dopamine- minimal effects at physiological concentrations
Glucagon – increase hepatic blood flow by vasodilatation
VIP & secretin – Vasodilate hepatic artery; no effects on portal vein
Angiotensin II- Vasoconstrict both
Vasopressin – Vasoconstrict and reduce portal blood flow
Increase hepatic blood flow
Feeding
Hypercapnia
Decrease hepatic blood flow
Spontaneous breathing – hepatic venous outflow reduced in inspiration and vice versa
Vigorous exercise – splanchnic vasoconstriction – reduced hepatic blood flow.
IPPV- reduced CO
Hypocapnia – increase resistance in portal system.
Hyperoxia- little effect
Hypoxia – initial increase return to baseline in 20 min.
Acute Haemorrhage
Portal venous flow reduced than hepatic arterial flow.
Increased oxygen extraction
Mobilize 50% of reservoir blood into systemic circulation by sympathetic stimulation.
Effect of anaesthetic agents
- Epidural & spinal – reduce total hepatic blood flow – reduced portal venous blood flow and MAP.
- Halothane – greatest reduction in total hepatic blood flow.Reduce hepatic arterial flow and portal blood flow. ‘Reduce buffer response’
- Enflurane- lesser reduction
- Isoflurane – reduced portal venous flow; normal or increased hepatic arterial flow;preserved buffer response
- TPS, etomidate, propofol
Dose dependent reduction in hepatic blood flow –
reduced CO and obtundation of buffer response.


