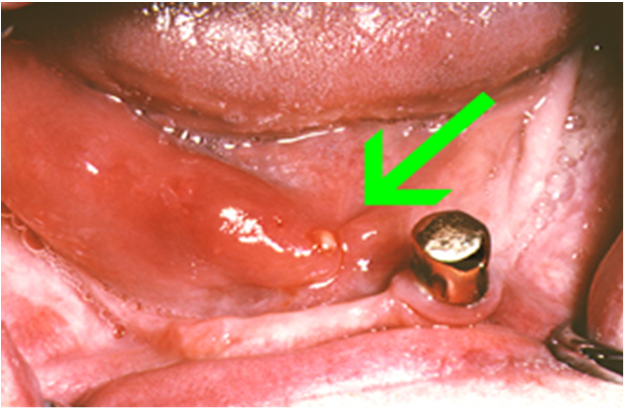
Sialolithiasis
There is presence of one or more round or oval calcified structures in the duct of the major or minor salivary glands( salivary stones)
How the stone is formed:

It is assumed that mucin proteins and desquamated ductal epithelial cells form a small nidus on which the calcium salts are precipitated, this nidus then allows concentric lamellar crystallizations to occur and thus sialolith increases in size as a layer by layer gets deposited on it
Clinical features of sialolithiasis:
About 80%of sialolith affects the major salivary glands and there is more predilections for the submandibular gland.
Stones are rare in children the average age is the 4th decade with no sex preference.
They are asymptomatic discovered on dental radiographs.
If symptomatic the chief complains are pain and swelling . Swelling is results as there is ductal dilatation caused by the ductal blockade.
The pain is described as pulling drawing or stinging.
Sialolithiasis Investigations:
Panoramic radiograph.
Ultra sound imaging
orsailography
Histopathology of sialolithiasis:
Stone: On gross examination most stones are yellow or white in colour. they may be round to oval
- some of the stones are nodular
- after decalcification the stone shows concentric rings as of the annual rings of a tree trunk
-The stone is acellular and amorphous in nature and may contain microbial colonies.
Ducts: the ductal lining that surrounds sialolith shows variety of reactive changes.
- there is squamous and mucus cell
metaplasia and changes to stratified squamous epithelium with numerous mucous goblet cells


Sialolithiasis treatment:
- Many of the major salivary gland sialoliths can be removed by manipulation of the stone through major duct orifice
- When manipulation fails then a surgical cut is made into the main duct
- In triangular, or multiple stones and long standing obstructions removal of the stone and sialadenectomy is done.



No comments:
Post a Comment