Pathologic calcification of soft tissues occurs when calcium
and other mineral salts are deposited in a tissue or in a passage. There are
three types of pathologic calcifications: 1) Dystrophic calcification is that
which occurs in degenerating and dead tissues. Calcificationof the larval stage
of tapeworm (cysticercus) is an example of dystrophic calcification. 2)Metastatic
calcification is that in which calcium (and other) salts are deposited in
previouslyundamaged tissue as a result of an excess of salts in the circulating
blood.Hyperparathyroidism is an example of metastatic calcification which
occurs in kidneys andblood vessels. 3) Calcinosis is calcification that occurs
in or under the skin. Scleroderma,myositis ossificans, and multiple miliary
osteomas are examples of calcinosis.

SIALOLITH
A sialolith is a stone (salivary calculus) within a salivary
gland or duct. The formation of a sialolith is called sialolithiasis and occurs
as a result of precipitation of calcium andphosphate salts around a nidus of
mucous or bacterial debris. Sialoliths occur as single or multiple stones and
can cause swelling and pain. The pain is experienced during salivary stimulation
and is intensified at mealtimes. The accumulation of saliva in the gland produces
swelling and the gland becomes enlarged and firm. The pain is produced as a result
of the buildup of pressure due to the accumulation of saliva behind the stone.
The pain gradually subsides and the swelling diminishes because the stone
usually does not completely block the flow of saliva. If a sialolith is small
or does not obstruct the flow of saliva, there may be an absence of pain and
swelling. Most stones are found in the submandibular duct (Wharton's) and gland
than in the parotid duct (Stensen's) and gland because of the viscous
consistency and mineral content of the saliva from the submandibular gland and
the long, irregular length of the Wharton's duct.
The best radiographic projection for visualizing sialoliths
in the submandibular duct and gland is the standard mandibular occlusal view.
Occasionally, sialoliths are seen incidentally on periapical radiographs, in
which case they may be misdiagnosed as osteosclerosis. To differentiate a
sialolith from an osteosclerosis, use the Clark's rule of tube-shift technique
to localize objects, that is, to find the bucco-lingual relationship. Stones in
the parotid duct and gland are best demonstrated by placing a periapical film
in the buccal vestibule and x-radiating them with a reduced exposure time.
Approximately 20% to 40% of all sialoliths are radiolucent. When this is
suspected, sialography (injection of a radiopaque dye into the ductal opening
and then x-radiating them) must be undertaken to visualize the stones. The duct
or gland injected with the radiopaque dye shows the radiolucent sialolith as a
non-filling defect. A sialolith must be differentiated from other soft tissue
calcifications, especially from a calcified lymph node. The latter is usually asymptomatic
and sialography may be required to distinguish the two lesions.


Fig 11-1 Mandibular occlusal projection shows a sialolith
(salivary calculus) in the duct of the submandibular gland (Wharton's duct).
The patient has a history of pain and swelling in the salivary gland which is
intensified at mealtime when saliva flow is stimulated. The pain gradually
subsides and swelling diminishes because the stone usually does not completely
block the flow of saliva.


Fig. 11-2 On periapical radiographs, the radiopacity may be
misdiagnosed as osteosclerosis. To differentiate an osteosclerosis from a
sialolith, take two radiographs using different vertical (or horizontal)
angulations of the x-ray beam. If the radiopacity changes its position in
relation to the adjoining teeth, as shown here, the radiopacity is a sialolith
in the floor of the oral cavity (Clark's rule: same lingual, opposite buccal).
Another method to identify a submandibular sialolith is to take an occlusal
projection.


Fig. 11-3 A sialolith on a panoramic radiograph may be
misdiagnosed as a calcified lymph node. In the absence of clinical signs and
symptoms it is difficult to differentiate the two types of calcifications
unless a sialogram is made.


Fig. 11-4 Sialogram showing an obstruction in the Wharton's
duct preventing the flow of the radiopaque dye into the submandibular salivary
gland. The stone (arrow) is blended with the radiopaque dye.
CALCIFIED LYMPH NODE
A calcified lymph node is indicative of a prior chronic
infection involving the node. A history of successfully treated tuberculosis is
often associated with this calcification. The condition is asymptomatic. It may
involve a single node or a chain of submandibular or cervical nodes. The
calcified superficial lymph nodes are palpable as bony, hard, round or linear masses
with variable mobility. They are often observed on a panoramic radiograph,
where they may appear below the inferior border of the mandible and near the
angle of the mandible. Calcified lymph nodes are often found incidentally on
radiographic examinationsSome may be radiographically projected over the
mandibular bone and may be misdiagnosed as osseous lesions.
A calcified submandibular lymph node may be difficult to
distinguish from a sialolith. The former is invariably asymptomatic whereas the
latter is frequently accompanied by pain and swelling at mealtimes. Sialography
may be required to distinguish the two lesions.


Fig. 11-5 Calcified lymph nodes located inferior to the
angle of the mandible. Priorchronic infection of the lymph nodes may result in
calcification of the nodes. A history of successfully treated tuberculosis is
often associated with this calcification. This asymptomatic condition may
involve a single node or a chain of nodes.


Fig. 11-6 A lateral cervical radiograph shows a chain of
calcified lymph nodes.
PHLEBOLITH
Phleboliths are calcified thrombi that occur in veins or
sinusoidal vessels of hemangiomas involving the soft tissues adjacent to the
jaws. On a radiograph they appear as round or oval bodies which may exhibit
concentric calcific rings similar to the cross section of an onion. Phleboliths
may occur singly or as multiple calcifications. On periapical radiographs,
calcifications may be superimposed on the mandible and thus misdiagnosed as
osseous lesions within the jaw or as sialoliths.

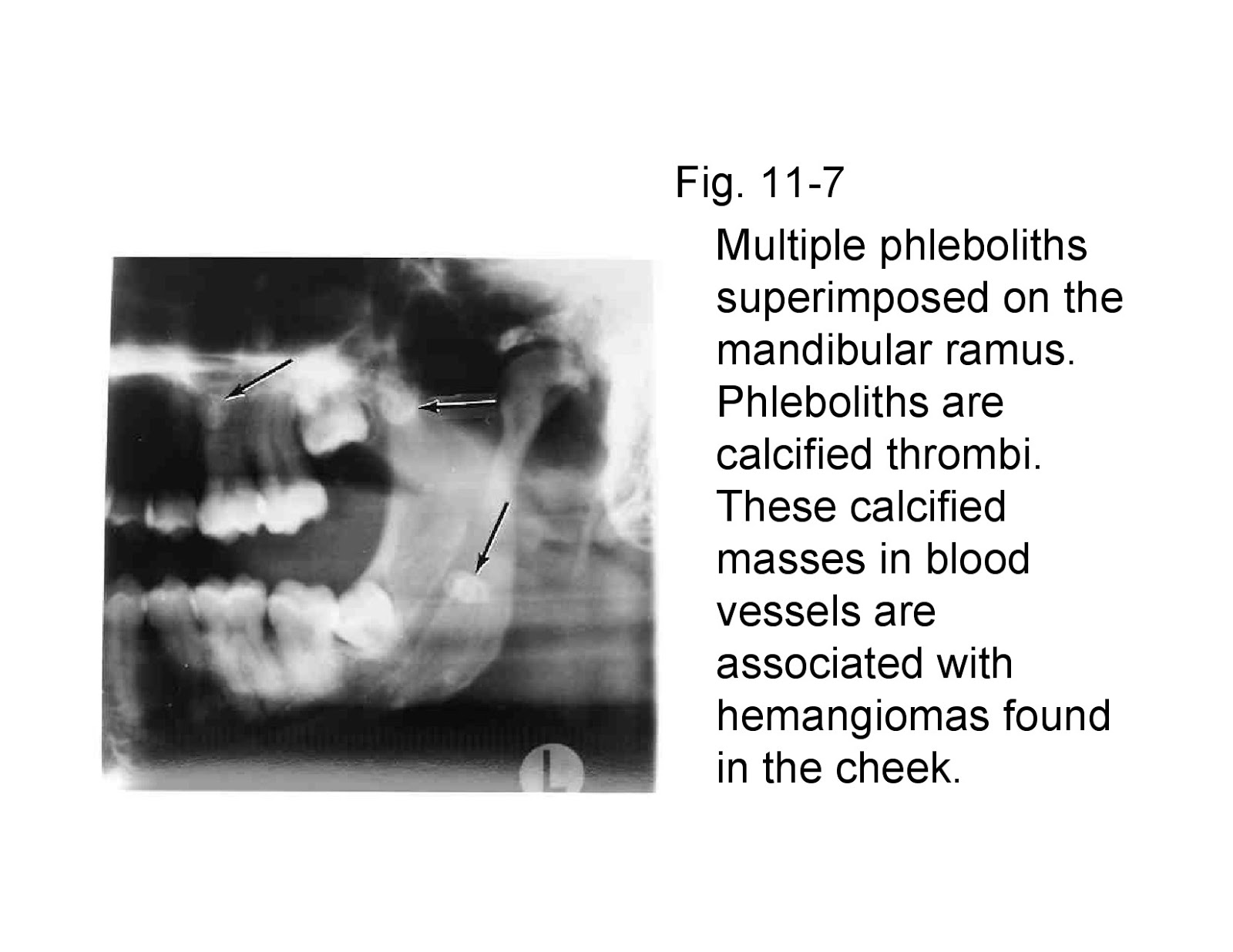
Fig. 11-7 Multiple phleboliths superimposed on the
mandibular ramus. Phleboliths are calcified thrombi. These calcified masses in
blood vessels are associated with hemangiomas found in the cheek.


Fig. 11-8 Multiple phleboliths of various sizes in cavernous
hemangioma of the face. The radiograph is of the patient's cheek.
CALCIFICATION OF ARTERIES
Calcification of the walls of arteries occurs in
arteriosclerosis and in secondary inflammatory conditions involving arteries.
The calcium salts are deposited within the medial coat of the vessels.
Calcification can occur in a number of arteries of the body (iliac, femoral,
abdominal aorta, etc.), however, in the facial region the facial artery is the
one that is often involved. Calcified arteries of the cheek and oral cavity may
appear as faint images on periapical radiographs. In the Sturge-Weber syndrome
(capillary hemangiomas of the face, oral mucosa, and cranium), the cranial
hemangiomas often show marked calcification of the blood vessels.


Fig. 11-9 Calcification of the facial artery. It may occur
in arteriosclerosis and represents an inflammatory process.


Fig. 11-10 Calcification of the facial artery. The
radiopacity of the artery is the result of deposition of calcium salts within
the medial coat of the vessel.
ANTROLITH
A calcified mass in the maxillary sinus is called an
antrolith. It is produced by calcification of a nidus which may be a bone chip,
root fragment, foreign object, or stagnant mucus in sites of previous inflammation.
Most of the antroliths are asymptomatic and are detected incidentally on
radiographic examinations. However, on rare occasions when an antrolith continues
to grow and become very large, it may be associated with sinusitis. Antroliths must
be differentiated from root fragments in the maxillary sinus. A root fragment
will show the root anatomy such as the presence of a pulp canal in a
cone-shaped (root-shaped) radiopacity. When calcification comparable to an
antrolith occurs in the nasal fossa, it is called a rhinolith.


Fig. 11-11 Calcified mass in the maxillary sinus is called
an antrolith. A foreign object, bone chip, root fragment or stagnant mucus acts
as a nidus for calcific deposits. It is usually asymptomatic.


Fig. 11-12 Antrolith (stone in maxillary sinus) on the floor
of the sinus. It is asymptomatic.
MULTIPLE MILLIARY OSTEOMAS OF SKIN
(Osteoma cutis, calcinosis cutis)
Multiple milliary osteomas of skin, also known as calcinosis
cutis, are situated in the cutis and subcutis. Some of these calcifications are
associated with acne or some other form of dermatosis. They are found
incidentally on radiographic examinations. They appear as doughnut-shaped
radiopacities with radiolucent centers which represent the central marrow cavities.
Multiple miliary osteomas are imaged better by placing a dental film in the vestibules
and against the inside surface of the cheek and using a reduced exposure time.


Fig. 11-13 Multiple miliary osteomas of skin are soft tissue
calcifications of skin. Some are reported to be associated with acne or some
other form of dermatosis.


Fig. 11-14 Calcinosis cutis showing doughnut-shaped
radiopacities.
CALCIFIED STYLOHYOID LIGAMENT AND EAGLE'S SYNDROME
Calcification of the stylohyoid ligament may sometimes be
found incidentally on a panoramic radiograph and located posterior to the ramus
of the mandible. It may occur unilaterally or bilaterally. In about 50% of the
cases, the individuals are asymptomatic. In those cases associated with pain
and discomfort, the entity is called "Eagle's syndrome".
The syndrome includes vague pain on mandibular movements
such as swallowing (dysphagia), turning the head or opening the mouth,
sensation of foreign body in throat, and constant dull ache in the throat.
Other symptoms include headache, earache (otalgia), dizziness, pain in
temporomandibular joint area and also in the base of the tongue or transient
syncope. The symptoms are probably caused by the elongated styloid process impinging
on the glossopharyngeal nerve. When the jaws are closed, the pain subsides in some
of the cases. It is important for the dentist to be aware that pain associated
with calcified stylohyoid ligament may simulate pain associated with that of the
temporomandibular joint.
On a radiograph, the calcified stylohyoid ligament appears
as a thin, long, tapering radiopaque process extending downwards from the
styloid process. Sometimes it may extend up to the lesser horn of the hyoid
bone. The farther the mineralized ligament extends towards the hyoid bone, the
more likely it is that it will be interrupted by radiolucent joint like
junctions. Surgical resection is required in patients exhibiting symptoms.


Fig. 11-15A Patient with Eagle’s syndrome. The stylohyoid
ligaments are bilaterally calcified. Patient complained of constant dull ache
in the throat, pain on turning the head, and pain in the vicinity of the
temporomandibular joints.
Fig. 11-15B Calcified stylohyoid ligament. Sometimes, this
calcification may be associated with Eagle's syndrome. The syndrome produces
cervical pain on turning the head, upon swallowing and on opening the mouth.
The patient may have headaches, and dizziness.


Fig. 11-17 Bilateral calcified stylohyoid ligament in a case
associated with Eagle's syndrome.

CALCIFIED THYROID CARTILAGE
Calcification of the thyroid cartilage is normal and
increases with age. The thyroid and cricoid cartilages have been found to
undergo a greater frequency of calcification in the female population, but a
higher degree of ossification has been noted in male subjects. (In the hyaline
cartilages of the larynx, calcification does not always precede ossification
and there is little correlation between the two).


Fig. 11-18 Calcification of the thyroid cartilage. It is
asymptomatic.
MYOSITIS OSSIFICANS
In myositis ossificans, bony structures such as lamellae,
lacunae and marrow are deposited in soft tissue. The cause of this ossification
in muscles, ligaments, tendons and fascia is unknown. It may be caused by
trauma or heavy muscular strain that occurs in certain
occupations and sports. During the healing process, the
blood in the traumatized region gets organized and later calcified. The
calcification takes place in the connective tissues around the muscles. The
digastric, masseter, temporal and sternomastoid are usually involved. The
patient finds it difficult to open the jaws when the muscles of mastication are
involved. The characteristic radiographic appearance is that of strand-like
calcifications along the long axis of the muscle fibers.
CYSTICERCOSIS
Cysticercosis is a helminthic (parasitic worms) disease
which completes the larval phase of its life cycle in the pig. When an
individual ingests eggs of the (pork) tapeworms from contaminated water or
food, the larval form of the tapeworms are hatched in the gastrointestinal
tract, and enter the vascular and lymphatic systems. They are then deposited in
various tissues and organs of the body. At this stage, there is no radiographic
evidence of their presence. After their death, the larval spaces are filled
with fibrous tissue which later becomes calcified. These calcifications in
muscle and subcutaneous tissue are visible on a radiograph as multiple
radiopaque ovoid or elliptical objects.
Fig. 11-19 Radiograph of patient with cysticercosis. The
calcified encysted larvae are seen in the soft tissues at the back of the neck
and a single one is seen in the area of Wharton’s duct.





No comments:
Post a Comment