Blood supply
Arterial supply
• Subclavian artery(neck)
• Axillary artery( upper arm: upto lower border of teres major)
• Brachial artery (lower part of arm)
• Radial artery (lateral)
• Ulnar artery( medial),common interosseous
• Palmar arches
• Digital

The subclavian artery becomes the axillary artery after crossing the 1st rib
The axillary artery becomes the brachial artery after crossing the posterior axillary fold
The brachial artery divides just distal to the elbow into the radial and ulnar arteries.
The ulnar artery gives rise to the common interosseous artery, which divides into anterior and posterior interosseous arteries.
The hand is supplied on the palmar aspect by variable anastomoses between branches of the radial and ulnar arteries.
Brachial artery
Begins at the distal border of the tendon of teres major
Ends about 1 cm distal to the elbow joint by dividing into radial and ulnar arteries.
Branches :
· Profunda brachii artery
· Nutrient artery of humerus
· Superior ulnar collateral artery
· Middle ulnar collateral artery (if present)
· Inferior ulnar collateral artery
· Muscular branches
Radial artery
Begins from the brachial artery near the neck of the radius
· Passes deep to brachioradialis
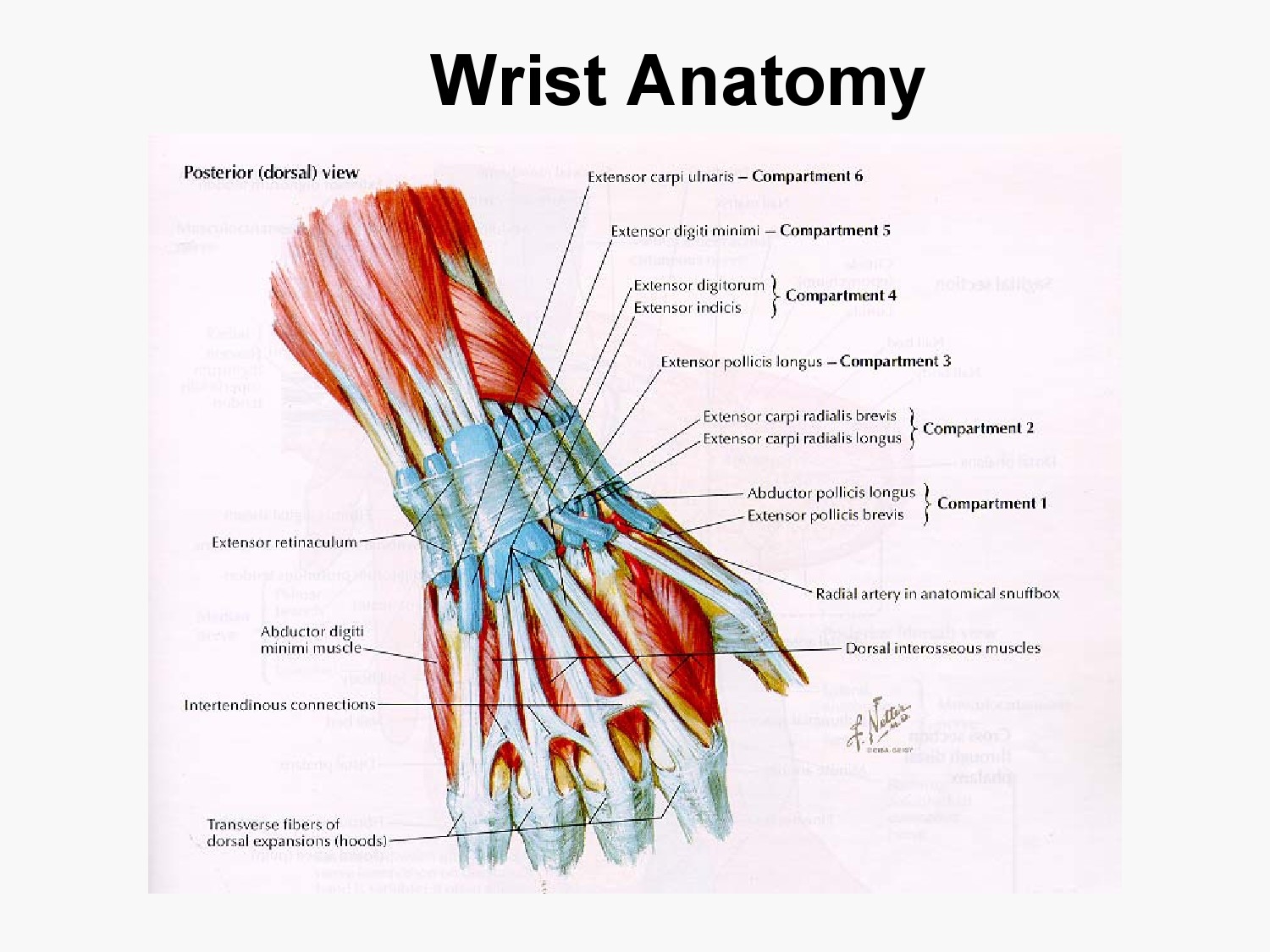
· At the wrist it passes in the anatomical snuff box
· Ends in the hand by anastomosis with the deep branch of the ulnar artery,
· completing the deep palmar arch
Branches :
· Radial recurrent artery (anastomoses with the radial collateral branch of the profunda brachii)
· Muscular branches
· Cutaneous branches
Ulnar artery
Begins from the brachial artery near the neck of the radius
passes deep to pronator teres, flexor carpi radialis, palmaris longus and flexor digitorum superficialis
The ulnar head of pronator teres separates it from the median nerve
At the wrist it passes in the anatomical snuff box
Ends in the hand by anastomosis with the superficial palmar branch of the radial artery, completing the superficial palmar arch.
Branches :
· Anterior ulnar recurrent artery
· Posterior ulnar recurrent artery
· Common interosseous artery, which divides into anterior interosseous artery and posterior interosseous artery (which gives rise to the posterior interosseous recurrent artery) .
· Muscular branches
· Cutaneous branches along the septum between flexor carpi ulnaris and flexor digitorum superficialis.
Anterior interosseous artery
Begins at the proximal border of the interosseous membrane
Descends on the anterior aspect of the interosseous membrane with the anterior interosseous branch of the median nerve, between the contiguous sides of flexor digitorum profundus and flexor pollicis longus.
Pierces the interosseous membrane proximal to pronator quadratus
Distally it anastomoses with the posterior interosseous artery and the dorsal carpal arch.
Branches :
· Median artery
· Muscular branches for FDP, FPL, pronator quadratus, and deep extensor muscles
· Small cutaneous branches for the lower lateral border of the forearm
Posterior interosseous artery
Begins at the proximal border of the interosseous membrane
Passes dorsally between supinator and abductor pollicis longus
Descends deep in the groove between extensor carpi ulnaris and extensor digiti minimi
Distally it anastomoses with the terminal part of the anterior interosseous artery and the dorsal carpal arch.
Branches :
· Multiple muscular branches
· Fascio-cutaneous branches in the intermuscular septum
Veins of upper limb
Superficial veins
- Dorsal venous network
- Cephalic vein
- Basilic vein
- Axillary vein( basilic+ brachial vein)
- Median cubital vein
- Median vein of forearm
Deep veins
- Named according to companian arteries
- Radial vein
- Ulnar vein
- Brachial vein
- Axillary vein
Veins
The venous drainage of the upper limb is composed of superficial and deep vessels.
The deep veins accompany the arteries. They are connected to the superficial system by perforating veins.
The superficial veins starts on the back of the hand as a dorsal arch.
•The cephalic vein begins at the radial extremity of the arch. It ascends along the lateral aspect of the arm, then it pierces the deep fascia to enter the axillary vein just distal to the clavicle.
•The basilic vein passes along the medial aspect of the forearm, pierces the deep fascia at the elbow and joins the venae comitantes of the brachial artery
•The median cubital vein links the cephalic and basilic veins in front of the elbow.

Surface anatomy-Important landmarks of upper limb
• Acromion
• Clavicle
• Deltoid ( im injections)
• Humerus
• Biceps muscle
• Biciptal groove
• Brachila pulse( blood pressure)
• Triceps
• Olecrnon process( pt of the elbow)
• Medial /lateral epicondyles
• Triangle
• Cubital fossa
• Median cubital vein- iv
• Cephalic vein
• Ulna
• Radius
• Styloid process
• Radial artery( pulse)
• Ulnar artery
• Anatomical snuff box
• Thenar eminenc
• Hypothenar eminence
• Carpal tunnel


 |
| Cubital Fossa |




 |
| Styloid process |














Axilla( armpit)
• Pyramidal space between the upper lateral chest and the innerside of the arm
• Boundaries
-Apex –( between the clavicle,scapula and 1st rib)
-Base-(axillary fascia)
-Anterior ( pectoralis major and minor muscles)
-Posterior ( subscapularis,latissimus dorsi and teres major)
Medial- ( first 4 ribs and serratus anterior muscle)
Lateral-( bicepetal groove of the humerus)
• Contents
-Axillary lymph nodes
-Axillary artery /vein
-Brachial plexus
Brachial plexus
Plexus- is a network of nerves
Brachial plexus-
• Found in the neck and axilla
• Formed by ventral rami of c5- c8 and t1 ( there may be contributions from c4, t2)
• Gives rise to nerves that supply the upper limb
Formation
• Roots- C5-C8 and ti ( ventral rami)
• Trunks-upper , middle, lower
• Divisons-anterior and posterior
• Cords-medial,lateral and posterior
Axilla Brachial plexus pics
Nerves arising from the cords
Medial cord
· Medial cutaneous nerve of arm- cutaneous supply to skin· Medial cutaneous nerve of forearm-cutaneous supply to the skin· Medial root of medial nerve- joins with lateral root to form median nerve· Ulnar nerve· Medial pectoral nerve
Lateral cord
· Lateral root of median nerve· Musculocutaneous nerve· Lateral pectoral nerve
Nerves from the posterior cord
• Upper subscapular nerve
• lower subscapular nerve
• thoracodorsal nerve
• Radial nerve
• Axillary nerve




Important nerves and area of supply
1. Median nerve( formed from both medial and lateral cord)-
A) Supplies all the flexors of the forearm( except flexor carpi ulnaris and medial half of fdp)
B) Intrinsic muscles in the lateral palm including thenar eminence)
2. Ulnar nerve
A) Supplies the medial half of fdp and the flexor carpi ulnaris
B) Supplies most of the intrinsic muscles of the hand including the hypothenar eminence, and skin on the medial side of the hand
Clinical application
injury to median nerve-” ape hand”
Injury to ulnar nerve-” claw hand”
Musculocutaneous nerve
A) Supplies the biceps, coracobrachialis and brachialis
Axillary nerve
- Supplies the deltoid and teres minor muscle
- Supplies the shoulder joint
Radial nerve
- Supplies the triceps
- Supplies the brachioradialis
- Supplies most of the extensors of the forearm
- * injury results in “ wrist drop”
Carpal tunnel
• Tunnel formed between the concavity of the carpal bones and a ligament that covers this( flexor retinaculam)
• Tendons of the flexors pass through
• Median nerve also passes through
• Crowded tunnel
Carpal tunnel syndrome
- Caused due to compression of the nerve in the tunnel
- Causes-
- 1. Swelling of the tedons( overuse)
- 2. Pregnancy( edema)
- 3. Arthritis
Symptoms- tingling or numbness-lateral part of hand, weakness in thumb movement
Treatment- rest, splinting,anti-inflammatory drugs, surgery
Peripheral Nerve Injuries of the Upper Limb
Radiculopathy
• Process affecting the nerve root, most commonly by a herniated disc
– Weakness in muscles supplied by the nerve root (myotome)
– Sensory loss in the area of the skin supplied by the nerve root (dermatome)
Mononeuropathy
• Dysfunction of a single peripheral nerve
– Weakness in muscles supplied by the nerve
– Sensory loss in the area of the skin supplied by the cutaneous branches of the nerve
Brachial Plexopathy
• Can refer to involvement of the entire plexus, or parts of the plexus
– Trunk lesion
– Cord lesion
• Distribution of weakness and numbness depends upon the part of the plexus affected
Sensory Supply to the Arm
• Because fibers from different nerve roots come together and then split apart in the plexus
– A dermatome may include areas of the skin supplied by different peripheral nerves
– A single nerve may supply sensation to skin covered by more than one dermatome
• Because of the pattern of root contribution to the plexus:
– An upper trunk lesion has sensory loss in the combined C5,6 dermatomes
– A middle trunk lesion has sensory loss in the C7 dermatome
– A lower trunk lesion has sensory loss in the combined C8T1 dermatomes
 |
| Dermatomes of anterior arm |
 |
| Dermatomes of the Posterior Arm |
Principles of Localization
Certain sites are prone to nerve entrapments/injuries
– Nerve opposing bone
• Ulnar nerve at the elbow
– Closed spaces
• Carpal tunnel
– Adjacent structures
• Median nerve at the elbow, adjacent to the brachial artery
• Order in which branches arise
• Movements at specific joints
– Single nerve
• Elbow extension
• Radial
– Multiple nerves
• Elbow flexion
• Musculocutaneous
• Radial
Median nerve injuries
Median Nerve.
• The median nerve enters the palm via the carpal tunnel, running between the flexor digitorum superficialis (FDS) and flexor carpi radialis (FCR). At the proximal border of the transverse carpal ligament (TCL), it gives off a palmer cutaneous branch (PCB) from its radial border running between the palmaris longus and FCR that provides sensation to the thenar skin. The PCB of the median nerve is at risk for injury during carpal tunnel surgery. At the distal border of the TCL, the median nerve divides into 5 or 6 branches: the recurrent motor branch to the muscles of the thenar eminence, a common digital nerve for the thumb, the proper digital nerve for the radial side of the index finger, and two common digital nerves for the adjacent areas of the index and long, and long and ring fingers respectively. The origin of the recurrent motor branch varies with respect to the TCL, with the majority being extraligamentous. It is responsible for innervating the superficial head of the FPB, the abductor pollicis brevis (APB), the opponens pollicis, and the two radial lumbricals.
Entrapment of Median nerve Can Occur at :
1) Course in the arm
• supracondylar process
2) At the elbow
3) in the forearm
- lacertus fibrosus
- pronator teres
- sublimis bridge
4) at the wrist
5) In the hand
Median injury produces
· paralysis of the muscles supplied by it
· deformity of the hand
· loss of sensation
Above The Elbow-Motor Affection
(1) Paralysis of all muscles supplied .
(2) Loss of pronation of the forearm .
(3) Weak flexion of the wrist .
(4) Loss of the flexion & opposition of the thumb.
Deformity: Ape Hand Deformity
(1) Hyper-extended thumb .
(2) Adduction .
(3) Flat thenar eminence.
Sensory Loss
- Lat. 2/3 of the palm of the hand
- Lat. 3 ½ fingers anteriorly & their distal halves posteriorly.
Below The Elbow-Motor Affection :
-Paralysis of the 5 hand muscles supplied by the nerve.
-The forearm muscles escape the injury as they are supplied at elbow.
Deformity : Ape Hand Deformity
Sensory Loss :
-Lat. 2/3 of the palm of the hand.
-Lat. 3 ½ fingers anteriorly & their distal halves posteriorly.
Clinical Features
• Inability to flex IP joint of thumb
• Ape thumb deformity
• Oppones palsy
• Sensory signs
Carpal Tunnel Syndrome
Definition
It’s a Clinical Diagnose Of peripheral neuropathy, results from compression of the median nerve at the wrist



Clinical Features
· Pain
· Numbness
· Tingling
· Symptoms are usually worse at night and can awaken patients from sleep.
· difficulty in holding on to a glass or cup securely
· To relieve the symptoms, patients often “flick” their wrist as if shaking down a thermometer (Flick Sign).
· Pain and paresthesias may radiate to the forearm, elbow, and shoulder.
· Decreased grip strength may result in loss of dexterity, and thenar muscle atrophy may develop if the syndrome is severe.
Pronator Syndrome
- Proximal Forearm Compression
- Because Of :-
Ø ligament of Struthers,
Ø lacertus fibrosus,
Ø pronator teres muscle
Same Symptoms As C.T.S But Could Be Differentiated By :
• include the distribution of the palmar cutaneous nerve
• The Tinel sign is positive at the forearm level
• The Phalen maneuver does not provoke symptoms
• Patients may experience pain with resistance to contraction of the pronator teres or flexor digitorum superficialis
Anterior Interosseous Syndrome
Clinical Findings
ü inability to flex either the thumb interphalangeal joint or the index-finger distal interphalangeal joint .
ü In contrast to those with pronator syndrome, these patients do not complain of numbness or pain .



