Cyst is a pathological cavity lined by a epithelium and
containing fluid or semi solid material.
Classification of cyst of the jaws
Developmental cyst
Odontogenic
- Gingival cysts of infants (epstain pearls)
- Odontogenic kerato cyst(primodial cyst)
- Orthokeratinized odontogenic cyst
- Dentigerous (follicular cyst)
- Eruption cyst
- Lateral periodontal cyst
- Gingival cyst of adults
- Glandular odontogenic;sialoodontogenic cyst
Non-odontogenic cyst
- Nasopalatine duct cyst
- Nasolabial cyst
- Inflammatory odontogenic cyst
- Radicular
- Residual
- Lateral
- Paradental
Key features of jaw cysts
- Form sharply defined radiolucencies with smooth borders.
- Fluid may be aspirated and thin walled cysts may be trans illuminated.
- Grow slowly,displacing rather than resorbing teeth.
- Symptoms unless infected and are frequently chance radiographic findings.
- Rarely large enough to cause pathological fracture.
- Form compressible and fluctuent swellings if extending in to soft tissues.
- Appear bluish when close to the mucosal surface
Major factors in the pathogenisis of the cyst formation
- proliferation of epithelial lining and fibrous capsule
- hydrostatic pressure of cystic fluid
- resorption of surrounding bone.
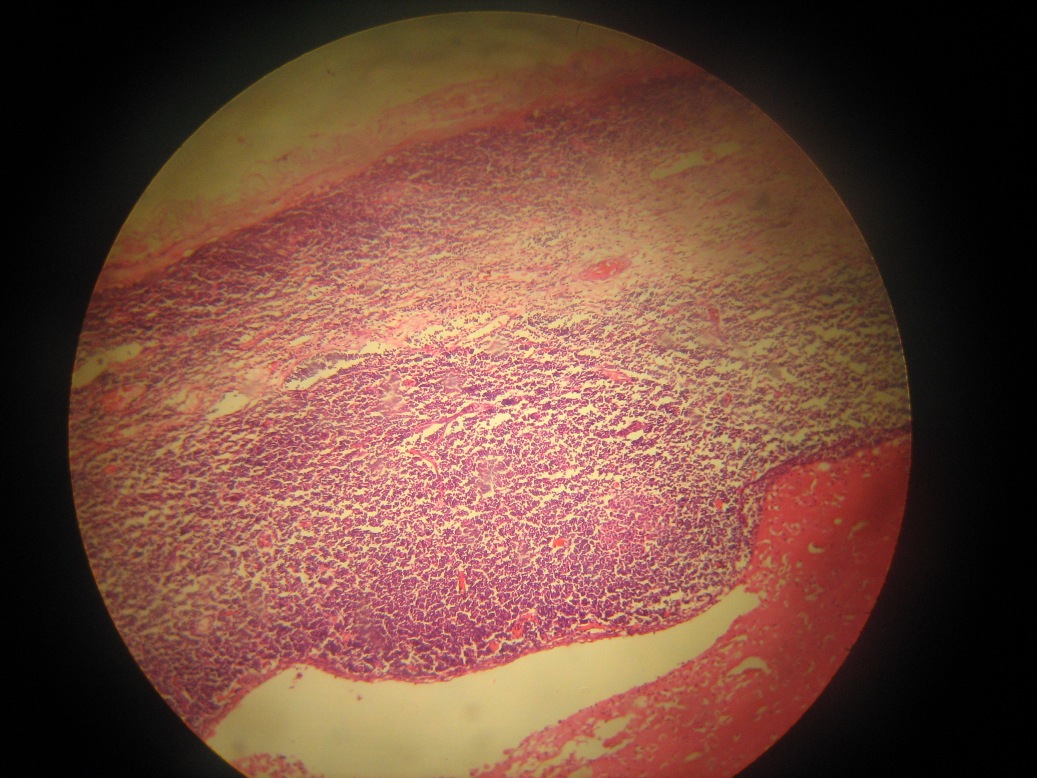
Periapical granuloma

- Sequalae of acute periapical periodontitis
- Ultimate resault of chronic periapical periodontitis-due to acute inflammation that has been inadequately drained and incompletely resolved.
- tooth is usually non vital
- First recognized as rounded area of radiolucency at the apex of the tooth-usually 5mm in diameter and well defined margins.
- Interprited as early cyst formation.
- Chronic periodontitis is typical chronic inflamation characterized by lymphocytes,plasma cells and macrophages.
- Infection is confined by inflammatory cells and granulation tissue surrounds the area.the granulation tissue grows into rounded mass forming granuloma.
- Osteoclasts resorb the bone to accomadate it.
- Spontaneous healing is absent due to tunnel of continuous infection in the root canal
- Variable degrees of proliferation of the epithelial rests of Malaassez in a periapical granuloma at the apex of the dead tooth are common.
- Epithelial proliferation may be sufficient to lead ultimately to cyst formation.
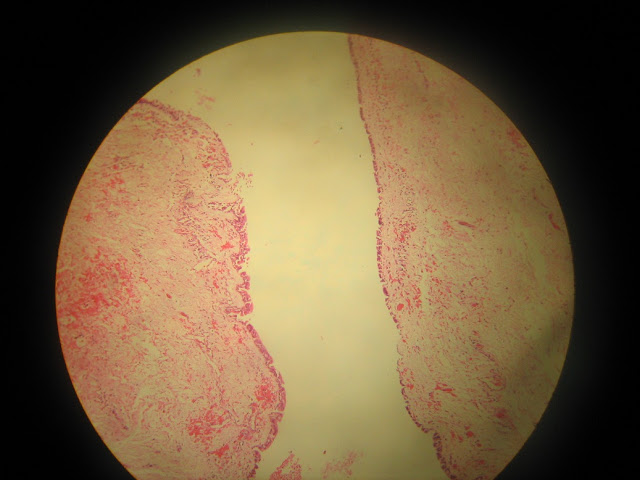
Radicular Cyst
- Most common type(Between 20-60yrs)
- Slowly progressing pain less swelling
- Pain and rapid exantion if inflammation/infection occurs.
- First swelling is hard,then become thinner and thinner.(creckling sensation->then fluctuent bluish colour swelling when par of the wall is entirely resorbed.
- Epithelium derived from-epithelial cell rests of malassez-stratified squamous epithelium.Hyaline/Rushton bodies may be seen in the epi.
- Cyst capsule-Colagenous fibrous connective tissue.
- Clefts-within the cyst capsule there are often areas split up by the fine needle shaped clefts.
key features

- form in bone in relation to the root of non vital tooth
- arise by epithelial proliferation in an apical granuloma
- usually asymptomatic unless infected
- Diagnosis-radiograph+non vital tooth+histology
- Do not recur after complete enucleation
- Residual cysts can remain after the causative tooth has been extracted and diagnosis is then less obvious
- Cholesterol crystals often seen in the cyst fluid but not specific to radicular cyst.
Dentigerous Cyst

- Arises in the bone and surrounds the crown of the tooth and is a dilation of the follicle.
- Attached to the neck of the tooth.
- Dentigerous cyst can cause pain or no pain.
- Affected teeth id often displaced.
- commonly associated with unerupted third molars and canines.
- Diagnosis-Radiograph+histological
- May be mistaken radiographically for an odontogenic keratocyst or ameloblastoma.
- Respond to enucleation or masupialisation and do not recur after treatment.
- Occationally pseudoloculation as a resault of trabeculation or ridging of the bony wall can be seen.
- Slow growth causes sclerotic bony outline and well defined cortex.
- Lining of dentigerous cyst typycally consist of thin,sometimes bilaminar,stratified epithellium,frequently with numerous mucous cells.
- Epithelium may be occationally keratinized by metaplasia.
- Fibrous wall similar as Radicular cyst but inflammatory changes are typicaly absent.
Parakeratinized odontogenic cyst/Odontogenic keratocyst
Key features
- 5-11% of jaw cysts
- incident peaks in 2nd and 3rd decades.
- Form intraosseously,most frequently in the posterior alveolar ridge or angle of mandible.mandible 75%,predominantly premolar and molar region
- may grow round the tooth
- Sometimes multilocular radiographically
- Spread extensively along marrow spaces before expanding the jaw
- Frequently recur after enucleation
- Definitive diagnosis only by histopathologically,although clinical and radiographic features may help.
- May be confused with ameloblastoma or with dentigerous cysts radiographically.
- May be part of the basal cell naevus(Gorlin)synndrome
- usually multilocular
Typycal Histological features of odontogenic keratocyst
- Epithelial lining of uniform thickness
- Flat lower border of epithelium
- Clearly defined basal layer of tall cells in parakeratinized cysts
- Thin eosinophilic layer of para keratin
- Cyst lining typically much folded
- Epithelial lining weakly attached to the fibrous wall
- Thin fibrous wall
- Satellite cysts in the wall
- Inflammatory cells typically absent or scanty
Evidance that OKC may be neoplastic
- High proliferative activity of epithelial lining
- Caused by mutation or deletion of PTCH tumor supressor gene
- May contain defects of p16,p53 and other tumor suppressor gene
- Associated with other neoplasms in the basal cell nsevus syndrome
- infiltrative(agressive)growth pattern
- SCC may rearly develop within OKC
- Recurrance
Possible reasons recurrance of OKC
- Thin fragile linings,difficult to enucleate intact
- Finger like cyst extensions in to cancellous bone
- Satellite(daughter) cysts sometimes present in the wall
- More rapid proliferation of keratocyst epithelium
- Formation of additional cysts from other dental lamina remnants(pseudo recurrance)
- Inferior standered of surgical treatment
- possibly a neoplasm
Orthokeratinized Odontogenic(kerato) Cyst

- Less common than para keratinized type
- Lower proliferative activity
- No association between basal cell naevus syndrome
- Usually monolocular
Key features of Lateral periodontal cyst and varients
Lateral periodontal cyst

- Developmental cyst that form beside a vital tooth
- Usually seen ny chance in routine radiographs
- Resemble other odontogenic cysts radiographically,apart from position near the crest of the ridge
- Cause no symptoms but can erode through the bone to extend in to th gingiva
- Microscopically,the lining is squamous or cuboidal epithelium,frequently only one or two cells thick,sometimes with focal thickenings
- Some cells may have clear cytoplasm
- Respond to enucleation
- The relate tooth can be retained if healthy
Sialo-odontogenic cyst


- Also rare and with many features in common with botryoid odontogenic cysts
- Frequently multi locular
- Microscopically,pools of mucin and mucous cells present in the epithelium
- Has a strong tendancy to recur
- Should be consevatively excised
Non odontogenic cysts
Naso palatine duct cyst

- Arise from the epithelium of the nasopalatine duct in the incisive canal
- Epithelial ling is stratified squamous epithelium or ciliated columnar epithelium
- Mucos glands and neurovascular bundles often present in the wall
- Often asymptomatic,chance radiographic findings
- Form in a incisive canal region
- Arise from the vestiges of the naso palatine duct and may be lined by columnar respiratory epithelium
- The long sphenopalatine nerve and vessels may be present in the wall
- Can usually be recognized radiographically
- Histological examination necessary to exclude othe cyst types arising at the site
- Do not recur after enucleation
Nasolabial Cyst

- Very common cyst forms outside the bone in the soft tissues,deep to the nso labial fold
- Probably arising from remnants of the nasolabial duct
- Occatonally bilateral
- Lining-Pseudostratified columnar epithelium
- Treatment-Simple excision
- May be complicate if the cyst has perforated the nasal mucosa and discharged in to the nose.
Para Dental Cyst

- Occationally resault from inflammation around partially erupted teeth.
- Particularly mandibular 3rd molars
- Affects males predominantly 20-25yrs
- Affected tooth is vital but show pericoronitis
Histopathologically
- Resembles radicular cyst
- But more inflammatory infiltration in wall.
Dermoid Cyst

- Cyst of soft tissue
- Commnly occur sublingually
- Developmental abnormality or branchial arches/pharyngeal pouches
- Develop belween hyoid and jaw or many form immediatly beneththe tongue
- Filled with desquamated keratin(sometimes)giving a semisolid(salty) like consistancy.
- Have dermal appendages in the wall->give the name dermoid cyst
- Dermoid cyst is a form of cystic teratoma which is similar to structure of dermis
- Derived from embryonic germinal epithelium/acquired entrapted skin/mucosa
- Lined by stratified squamous epithelium and contain skin appendages such as sebaceous glands in CT wall
- Dermoid cysts in the head and neck region appearing symmetrical swellings in the floor of mouth
- There are presumed to derived by entrapment of epithelium remnents during closure of mandibular and hyoid branchial arches
- Sublingual type produce bulge in floor of mouth
- Submental type produce bulge in submental arch(dough-like on palpation)
Epidermoid Cyst

- Small epidermoid cysts may also be found in the tongue,soft palate,buccal mucosa and lips where they are considered to be acquired lesions resaulting from traumatic implantation of surface epithelium
- Simple lesions without skin appandages are epidermoid cysts
Aneurysmal bone Cyst

- Intra osseous lesions consist of blood filled cavernous spaces
- occur in some frequently in jaws and molar areaof younger individuals is the commenest site.
- rapidly expanding lesion
- X-ray multilocular radiolucency
- Thin fibrous CT wall and consist of many blood filled cavernous spaces
- False type of cyst.non epithelialized

Branchial Cyst
- Arising from branchial arch remnants
- it has also been called lymphoepithelial cyst suggesting it's origin from cystic transformation of epithelium entrapted in cervical lymphnodes
- BC originated from 2nd arch->lateral aspect of upper neck near anterior border of sernocledomastoid muscle or at the mandibular angle
- Lesion->circumscribed fluctuent mass
- Young adults no sexual prediction
- Small ones canbe found in the floor of the mouth,Clinically resembles mucous retention cysts
- lined by stratified squamous epithelium
- Occationally columnar or cuboidal
- Cyst wall is composed of lymphoid tissue with scattered germinal centre surrounded by CT.
Key Words : oral surgeons wisdom teeth extraction dental implant surgery doctor of dental surgery oral surgeon dental operation dental gum surgery wisdom tooth surgery dental surgery oral surgery doctor of dental surgery cosmetic dental surgery dental laser surgery cosmetic gum surgery laser gum surgery








